Most people with a stomach ulcer don’t know they have one. They know they have pain, a burning, gnawing discomfort somewhere between the chest and the navel, and they’ve been managing it with antacids for months. Sometimes the antacids help. Sometimes they don’t. The pattern keeps returning.
Stomach ulcer symptoms and acidity overlap enough to confuse anyone. But they behave differently in ways that matter. Knowing which one you’re actually dealing with changes whether you need a two-week medication course or an endoscopy and H. pylori eradication. That’s not a small difference.
How Do I Know If I Have a Stomach Ulcer or Acidity?
The clearest distinguishing feature is timing, specifically, the relationship between pain and food.
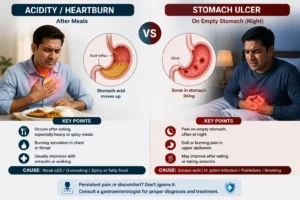
Acidity (GERD or gastritis) typically worsens after eating. Food triggers acid production, acid rises, chest burn follows. Lying down makes it worse. A glass of water or an antacid brings at least temporary relief. It’s an after-meal problem.
Stomach ulcer symptoms often follow the opposite pattern.
- Gastric ulcer pain (ulcer on the stomach wall): worsens shortly after eating, food triggers acid secretion that irritates the raw ulcer surface
- Duodenal ulcer pain (the more common type in India): classically occurs when the stomach is empty, 2–3 hours after meals, late at night, or early morning. Eating actually relieves it temporarily, because food buffers the acid making contact with the ulcer
That empty-stomach pain pattern, waking at 2am with a burning gnaw in the upper abdomen that a biscuit relieves, is peptic ulcer until proven otherwise. Not acidity. Not stress. And not something that resolves with long-term antacid use without addressing the underlying cause.
Common Stomach Ulcer Symptoms
Stomach ulcer symptoms exist on a spectrum, from mild and intermittent to severe and acute. Recognising the full range is what prevents months of misattribution.
Typical symptoms:
- Burning or gnawing upper abdominal pain, the central symptom; sits between the chest and navel, often described as a hollowness rather than a sharp pain. More of an ache than a burn.
- Empty-stomach pain, particularly duodenal ulcers; worse when fasting, before meals, or at night. Reliably relieved, at least temporarily, by eating or taking an antacid.
- Nausea, frequently present, particularly in the morning or during pain episodes
- Bloating and a sense of fullness, even after small meals; the inflamed stomach lining doesn’t tolerate volume well
- Loss of appetite, not always, but consistently present in active ulcer flares
- Burping and mild indigestion, present in both acidity and ulcers; not a distinguishing feature on its own
Symptoms that signal complications, see a specialist the same day:
- Black, tarry stools (melena), digested blood from a bleeding gastric ulcer passing through the gut; distinct smell, distinct colour. This is a medical emergency.
- Vomiting blood or coffee-ground material, upper GI bleed, requires immediate hospital assessment
- Sudden, severe stabbing abdominal pain that doesn’t resolve, possible perforation; life-threatening, needs emergency care
- Unexplained weight loss alongside persistent upper abdominal pain, always warrants endoscopy to rule out malignancy
Most stomach ulcer symptoms don’t reach the emergency threshold. But most patients also don’t recognise that persistent, recurring upper abdominal pain failing to respond to antacids is already a reason for a proper investigation, not more antacids.
H. Pylori Infection: The Cause Most Patients Don’t Know About
This is the part that changes the conversation entirely.
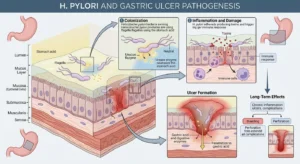
. pylori infection, Helicobacter pylori, is a bacterial infection of the stomach lining responsible for the majority of peptic ulcer cases globally, and for a disproportionately high percentage of cases in India. Estimates suggest more than half the Indian population carries H. pylori, largely through contaminated water and food.
Most carriers never develop ulcers. In a significant subset, the bacteria erodes the protective mucous layer of the stomach lining, creating the raw surface an ulcer sits on.
Why this matters for treatment:
- Without H. pylori eradication, ulcers recur, Antacids and PPIs (proton pump inhibitors) heal the ulcer surface but don’t eliminate the bacteria. The infection continues. The ulcer comes back, often within a year.
- H. pylori is directly treatable, a standard 2-week triple therapy (two antibiotics + a PPI) achieves eradication in the majority of patients. Confirmed eradication means a very low chance of ulcer recurrence.
- Long-term H. pylori infection is a known risk factor for gastric cancer, specifically gastric adenocarcinoma and gastric lymphoma. Not immediate. Not inevitable. But real enough that eradication is always the right call once infection is confirmed.
Testing for H. pylori is straightforward: a urea breath test, stool antigen test, or biopsy during endoscopy. The test takes minutes. The result changes the entire treatment approach.
How to Tell If It’s Acid Reflux or an Ulcer?
Both originate in the upper digestive tract. Both involve acid and discomfort. But they are mechanistically different, and that difference determines whether you need lifestyle changes, medication alone, or endoscopy and bacterial eradication.
Acid reflux (GERD):
- Burning sensation in the chest or throat, not deep abdominal pain
- Triggered by lying down, bending forward, large meals, spicy or fatty food
- Responds partially to antacids, PPIs, and dietary adjustments
- Worsens after eating, particularly late-night meals
- No blood in stool, no melena, no nocturnal pain pattern
Stomach ulcer symptoms:
- Pain is deeper, upper-middle abdomen, not chest; gnawing rather than burning
- Pattern is food-related but in the opposite direction, often worse on an empty stomach, relieved by eating (duodenal) or slightly worse post-meal (gastric)
- Antacids give temporary relief but don’t resolve the pattern, the pain keeps returning because the ulcer is still there
- Nocturnal pain (2–4am) is strongly associated with peptic ulcer, rarely with GERD
- Blood in stool, melena, or vomiting blood, red flags that never accompany simple acid reflux
The rule that matters most: if the pain pattern doesn’t fit standard GERD behaviour, if it’s worse on an empty stomach, wakes you at night, or isn’t responding to months of acid medication, the assumption should be peptic ulcer until an endoscopy says otherwise.
What Is the Difference Between Acidity and Ulcers?
Acidity and gastric ulcers are related but distinct conditions. The relationship is roughly: excess or dysregulated acid creates the environment; an ulcer is the physical wound that forms when that environment isn’t corrected, or when H. pylori infection erodes the protective barrier.
| Acidity (GERD/Gastritis) | Stomach Ulcer | |
| Cause | Acid reflux, dietary triggers, stress | H. pylori infection, NSAIDs, excess acid |
| Location of pain | Chest, upper-middle | Upper-middle abdomen, deeper |
| Pain timing | After meals | Empty stomach (duodenal) or after meals (gastric) |
| Responds to antacids | Yes, partially | Temporarily, but pattern recurs |
| Nocturnal pain | Uncommon | Common, classic duodenal pattern |
| Blood in stool | Never | Possible in complicated cases |
| Confirmed by | Clinical assessment, pH testing | Endoscopy with biopsy |
| Risk of complications | Low | Bleeding, perforation, malignancy if untreated |
Acidity is a functional problem, managed with lifestyle changes and medication. A stomach ulcer is a structural wound, it needs to be identified, its cause addressed (especially H. pylori), and then healed properly.
How Is a Stomach Ulcer Diagnosed? The Role of Endoscopy

Definitive diagnosis requires looking. Blood tests, H. pylori breath tests, and clinical assessment narrow the probability. But the stomach ulcer itself, its location, size, appearance, and whether biopsy is needed, is visible only through endoscopy.
Upper GI endoscopy (OGD scope):
A thin, flexible camera passed through the mouth into the oesophagus, stomach, and first part of the small intestine. In 20–30 minutes, it reveals:
- Active ulcer, its location, size, and signs of bleeding or healing
- Biopsy for H. pylori detection from the ulcer margin
- Exclusion of gastric cancer, critical when the ulcer has an unusual appearance or the patient is over 40
- Assessment of the surrounding stomach lining for gastritis or early damage
H. pylori testing options:
- Urea breath test, non-invasive, highly accurate; taken before treatment begins
- Stool antigen test, also non-invasive; useful for confirming eradication 4 weeks after completing treatment
- Biopsy at endoscopy, the most direct method when a scope is already being performed
Dr. Vibhor Pareek at Gastro Plus performs upper GI endoscopy with biopsy for H. pylori testing as part of comprehensive ulcer workup, so the diagnosis, the cause, and the biopsy happen in one procedure rather than across multiple visits.
Treatment Options for Stomach Ulcers
Treatment works well when it addresses both the ulcer and its cause.
For H. pylori-positive ulcers (majority of cases):
- Triple therapy, two antibiotics (typically clarithromycin + amoxicillin, or metronidazole-based regimens) plus a PPI, for 14 days
- Confirmation of eradication, urea breath test or stool antigen test 4 weeks after completing the course; skipping this step means not knowing whether the bacteria was actually cleared
- Continued PPI for 4–8 weeks after eradication to allow full stomach lining healing
For NSAID-induced ulcers:
- Discontinue or reduce the NSAID; switch to a gastroprotective alternative under guidance
- PPI for 8–12 weeks to heal acid erosion
- Long-term gastroprotection if the NSAID cannot be stopped
For complicated ulcers:
- Bleeding ulcer: endoscopic haemostasis, clips, cauterisation, or injection; IV PPIs post-procedure
- Perforation: urgent surgical intervention
- Gastric outlet obstruction from scarring: endoscopic dilatation or surgical bypass depending on severity
What doesn’t work as standalone treatment:
PPIs and antacids alone, without H. pylori eradication, produce temporary healing, and typically within 6–12 months, the ulcer returns. The bacteria is still there. The mucosal protection is still compromised.
The ulcer comes back. This is the most common reason for recurring stomach ulcer symptoms in patients who’ve “already been treated.”
According to WHO guidelines on H. pylori and gastric disease, confirmed eradication of H. pylori is the most effective single intervention for preventing peptic ulcer recurrence.
Conclusion
Stomach ulcer symptoms borrow the appearance of acidity, same region, same meal-related timing, same antacid reflex. But the underlying mechanism is different, the treatment is different, and the consequence of not treating it properly is a cycle of recurrence that ends with either a complication or a scope that finds what months of antacids missed.
The empty-stomach pain, the nocturnal gnawing, the antacids that work for a week and then don’t, that’s the pattern. It deserves an endoscopy, not another prescription pad. H. pylori infection is directly treatable. Peptic ulcers heal reliably when the cause is addressed.
The only thing that doesn’t work is continuing to manage a structural wound as if it’s a dietary problem.
That Recurring Upper Abdominal Pain Deserves a Definitive Diagnosis, Not a Longer Antacid Course.
An endoscopy takes 20–30 minutes and answers the questions that months of medication haven’t. At Gastro Plus, upper GI scoping is performed alongside H. pylori biopsy so the cause and the ulcer are confirmed in one visit, not across multiple referrals.
Dr. Vibhor Pareek and the Gastro Plus team offer:
- Upper GI endoscopy (OGD scope), diagnostic, with biopsy and H. pylori testing in the same procedure
- H. pylori diagnosis and eradication treatment, testing, therapy, and post-treatment confirmation
- Peptic ulcer management, complete treatment planning including medication, lifestyle guidance, and follow-up
- Bleeding ulcer endoscopic treatment, haemostasis procedures for complicated presentations
- Complete gastroenterology consultation in Gurgaon, for upper GI symptoms that haven’t been properly investigated
👉 Book a Consultation at Gastro Plus
Frequently Asked Questions
Q1. How to confirm if you have a stomach ulcer?
The definitive confirmation is upper GI endoscopy, the only way to directly visualise the ulcer, assess its severity, and test for H. pylori in the same procedure. Pre-endoscopy pointers that strongly suggest a peptic ulcer:
- Pain specifically worse on an empty stomach or at night
- No meaningful improvement with 4+ weeks of antacids or PPIs
- Black or tarry stools at any point, see a specialist the same day
Q2. Do you burp a lot with a stomach ulcer?
Excessive burping can occur with stomach ulcer symptoms but it’s not a defining feature, it’s also common in gastritis, GERD, and functional dyspepsia. What distinguishes ulcer-related burping: it tends to accompany the deeper abdominal discomfort rather than occurring independently,
and it doesn’t fully relieve the underlying pain the way gas-related burping does. Burping alone as an isolated symptom is rarely ulcer-specific.
Q3. Can stress cause a stomach ulcer?
Stress doesn’t directly cause peptic ulcer in the way H. pylori infection or NSAIDs do. However, it plays a real supporting role, stress increases acid secretion, delays gastric emptying, and can impair the mucosal repair mechanisms that protect the stomach lining.
“Stress ulcers” are a genuine clinical entity but occur in critically ill patients in ICU settings, not from everyday stress. What stress more reliably does is worsen existing stomach ulcer symptoms and slow healing.
Q4. Can a stomach ulcer heal on its own?
A small subset can, particularly if the triggering cause (an NSAID, a short-term stressor) is removed and the stomach gets relative rest. But H. pylori-positive ulcers do not reliably self-heal, and without eradication, recurrence within a year is common. The practical answer: don’t assume it will resolve.
If stomach ulcer symptoms are consistent for more than 2–3 weeks, investigation and treatment is the safer path than waiting.
Q5. What foods should I avoid with a stomach ulcer?
Foods that increase acid production or directly irritate the gastric ulcer surface:
- Spicy food, particularly raw chilli and pepper
- Caffeine, coffee, tea, energy drinks
- Alcohol, directly damages the stomach lining and impairs healing
- Carbonated drinks, highly acidic foods (vinegar-heavy dishes) Bland, smaller, more frequent meals reduce the acid load and give the ulcer surface more consistent buffering. This is supportive, not curative, the ulcer itself needs proper medical treatment.
Q6. What happens if a stomach ulcer is left untreated?
Untreated peptic ulcer can progress through a predictable complication pathway:
- Bleeding, the most common complication; slow bleeding causes anaemia, rapid bleeding requires emergency endoscopy
- Perforation, the ulcer erodes through the entire stomach or duodenal wall, causing sudden severe abdominal pain and requiring emergency surgery
- Gastric outlet obstruction, repeated scarring from healing ulcers can narrow the stomach exit, causing persistent vomiting
- Malignancy, long-term untreated H. pylori infection with chronic acid erosion is associated with gastric cancer risk over years