Pancreatitis symptoms usually begin with a sharp, persistent pain in the upper abdomen, one that radiates straight through to the back and gets noticeably worse after eating. The pancreas sits tucked behind the stomach, and it rarely gets suspected first. Most people assume gas, acidity, a pulled muscle, something they ate.
The problem is that pancreas inflammation doesn’t behave like those things. It’s more intense, more constant, and more insistent.
If the pain won’t let up, comes with nausea or vomiting, and feels worse lying flat, that’s not routine digestion trouble.
What Are the Early Symptoms of Pancreatitis?
Early pancreatitis symptoms are frustratingly easy to dismiss. They overlap with acidity, IBS, gastritis. That’s what delays diagnosis, not ignorance, just overlap.
The warning signs worth not writing off:
- Persistent upper abdominal pain, not cramps, not gas bubbles. A deep, constant ache in the upper middle or left abdomen, often worse after meals or alcohol. It doesn’t shift around the way gas does.
- Pain that radiates to the back, this is one of the more distinctive signals. When upper abdominal discomfort and back pain arrive together, especially post-meal, the pancreas deserves to be in the differential.
- Nausea and vomiting, in an acute flare, eating makes things dramatically worse. The body’s response is to reject.
- Fever and rapid heart rate, these suggest the pancreas inflammation has gone systemic, which is more urgent than localised discomfort.
- Swollen or tender abdomen, the area may feel hard or painful to light pressure.
- Oily, pale, foul-smelling stools, a chronic signal. When the pancreas stops producing enough digestive enzymes, fat passes through unabsorbed. This shows up in the stool before it shows up anywhere else.
In chronic cases, the symptoms are quieter, recurring dull discomfort rather than a dramatic attack, slow unexplained weight loss, indigestion that doesn’t respond to standard acid medications. Easy to live around. Harder to diagnose. More likely to be missed.
Acute vs Chronic Pancreatitis: What’s the Difference?
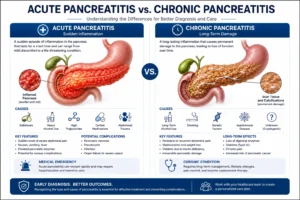
Two different conditions. Same organ. Partially overlapping symptoms. The distinction matters because treatment, urgency, and long-term impact are all different.
Acute pancreatitis is sudden onset. The pancreas flares, usually triggered by gallstones or alcohol, and the inflammation escalates rapidly. In mild cases it resolves in a few days with rest, fasting, and IV fluids. In severe cases,
it causes systemic complications and requires intensive hospital management. The pain arrives fast and demands attention.
Chronic pancreatitis is slow, cumulative damage. Often the result of repeated acute episodes, or years of heavy alcohol use, or both. Over time:
- Digestive enzyme production drops, causing malabsorption, particularly of fat
- Blood sugar regulation weakens as insulin-producing cells are damaged, sometimes progressing to diabetes
- Persistent low-grade pancreatic pain becomes a background feature of daily life
- Stools become fatty and difficult to flush (steatorrhea)
The difficult thing about chronic pancreatitis is that it doesn’t always announce itself dramatically. Some patients spend months managing “recurring indigestion,” unexplained weight loss, and mild upper abdominal discomfort before anyone investigates the pancreas specifically.
The subtlety is what makes it dangerous, it creates a long diagnostic gap.
Common Causes of Pancreatitis
Two causes account for the majority of cases. But the full list is longer, and the cause determines a lot about treatment.
Causes of acute pancreatitis:
- Gallstones, the most common single trigger. A stone lodges at the bile duct opening, blocks pancreatic drainage, and rapid inflammation follows
- Heavy alcohol use, even one significant episode can trigger a flare in susceptible individuals, not just chronic drinkers
- High triglyceride levels (hypertriglyceridemia), an underappreciated cause; levels above 1000 mg/dL carry significant risk
- Certain medications, some antibiotics, diuretics, and immunosuppressants are known pancreatic irritants
- Abdominal trauma or post-ERCP complications
- Autoimmune conditions, autoimmune pancreatitis, though less common, can mimic other causes
- Idiopathic, no identifiable cause in roughly 15–20% of cases, which is more common than most patients expect
Causes of chronic pancreatitis:
- Prolonged alcohol use (the leading cause)
- Repeated acute pancreatitis episodes that progressively scar the gland
- Hereditary or genetic mutations (PRSS1, SPINK1)
- Autoimmune pancreatitis
- Structural abnormalities or strictures in the pancreatic duct
Identifying the cause isn’t just academic, it directly changes what treatment looks like and whether recurrence can be meaningfully prevented.
How Do I Know If My Stomach Pain Is My Pancreas?
Most stomach pain isn’t the pancreas. But when it is, the pattern is specific enough to recognise, if you know what you’re looking for.
Pancreatic pain tends to:
- Sit in the upper middle or upper left abdomen, not lower abdominal cramping, not diffuse bloating
- Radiate through to the back, this is one of the most consistent features. Upper abdominal pain that connects to back discomfort, especially after eating, is a flag
- Worsen after meals, particularly fatty or heavy ones, because food triggers pancreatic enzyme secretion, which irritates an already inflamed gland
- Be constant, not spasmodic, gas pain comes and goes in waves. Pancreatic pain stays. It’s persistent, not rhythmic.
- Come with nausea or vomiting, especially in acute presentations
- Improve slightly when you lean forward or curl your knees to your chest, this is a known clinical sign, not just a comfort instinct
The pattern that often gets misread: upper abdominal pain after eating, chalked up to acidity, treated with antacids, no improvement. Acidity doesn’t radiate to the back. It doesn’t get worse with every meal regardless of what you take. If standard acid medication isn’t touching it, the pancreas is worth considering.
How Quickly Does Pancreatitis Pain Start?
In acute pancreatitis, pain comes on fast. Within hours of the trigger, a gallstone suddenly blocking drainage, a heavy night of drinking, a large fatty meal, the inflammation escalates rapidly.
The typical progression:
- Onset: A dull discomfort in the upper abdomen that builds quickly within 30–60 minutes
- Escalation: Intense, constant pancreatic pain within a few hours, severe enough that most people end up in an emergency room, not waiting for a next-day appointment
- Accompanying symptoms: Nausea, vomiting, and fever typically develop alongside the pain, not hours later, making the clinical picture hard to ignore
This rapid onset is why acute pancreatitis is so often diagnosed in emergency settings. The pain doesn’t allow waiting.
Chronic pancreatitis follows an entirely different timeline. The discomfort can begin as mild, recurring upper abdominal pain that builds over weeks or months, often misattributed to IBS, GERD, or gastritis long before the pancreas gets investigated.
This slow, quiet build is the more dangerous pattern, not because it’s more severe in the moment, but because it delays diagnosis by months and allows progressive damage to continue quietly.

When to Consult a Gastroenterologist
The threshold should be lower than most people set it. The pancreas is not an organ that rewards a “wait and see” approach once symptoms have started.
See a specialist immediately if:
- Upper abdominal pain is severe, constant, or radiating to the back
- Fever accompanies abdominal pain, this signals systemic inflammation, not just local discomfort
- Vomiting is persistent and you’re struggling to keep fluids down
- Jaundice appears (yellowing of skin or eyes with abdominal pain), this often indicates a bile duct obstruction, commonly from gallstones
- Stools have become consistently pale, oily, or unusually foul-smelling
Don’t wait for the dramatic pancreatitis symptoms if:
- You’ve had recurring mild upper abdominal discomfort for weeks with no clear cause
- Standard acidity or IBS treatment hasn’t worked
- You have a history of gallstones or heavy alcohol use and new digestive symptoms have appeared
Dr. Vibhor Pareek at Gastro Plus evaluates a significant number of patients who’ve been living with pancreatitis symptoms for months, diagnosed as acidity or functional gut issues, before a proper workup identified the pancreas. That gap matters because chronic pancreatitis progresses silently.
An early assessment, even for mild recurring discomfort, changes what’s still treatable.
Treatment Options for Pancreatitis symptoms
Treatment depends entirely on whether it’s acute or chronic, and what’s driving it.
For acute pancreatitis:
- Complete pancreatic rest, no food or drink initially, managed with IV fluids, pain control, and close monitoring. The pancreas needs to stop working temporarily to settle the inflammation.
- Addressing the cause, if gallstones triggered it, ERCP (Endoscopic Retrograde Cholangiopancreatography) or cholecystectomy (gallbladder removal) usually follows recovery. If alcohol is the cause, abstinence is non-negotiable and immediate.
- Managing complications, severe acute pancreatitis can lead to pseudocysts, necrotising pancreatitis, or multi-organ involvement. These need specialised gastro and surgical care.
For chronic pancreatitis:
- Enzyme replacement therapy (ERT), supplementing the digestive enzymes the pancreas can no longer produce, taken with every meal to restore proper fat and nutrient absorption
- Pain management, often the most complex part of chronic care, requiring a specialist approach rather than standard analgesics
- Dietary changes, low-fat diet, small frequent meals, and strict alcohol avoidance
- Diabetes management, if insulin production is compromised, this needs to be addressed specifically
- Endoscopic or surgical procedures, for duct strictures, stone removal, or persistent pain that doesn’t respond to conservative management
According to the NIH National Institute of Diabetes and Digestive and Kidney Diseases, early lifestyle intervention and proper treatment significantly reduce the risk of long-term complications from pancreatitis.
Conclusion
Pancreatitis symptoms don’t always arrive dramatically. Sometimes it’s a back ache that comes with every meal. Stools that quietly changed. Indigestion that never responded to antacids. None of these are alarming on their own, all of them matter when they’re consistent.
The pancreas is quiet until it isn’t. And when it stops being quiet, the pain is significant, fast, and hard to ignore. The goal is to catch the pattern before it becomes a crisis, when the options are still wide open and the damage is still reversible.
If something in your upper digestion has felt consistently off, that’s worth a proper evaluation. Not tomorrow. Soon.
Upper Abdominal Pain That Doesn’t Add Up? It’s Worth Evaluating Properly.
Pancreatitis is frequently misdiagnosed as acidity, IBS, or gastritis, sometimes for months. If recurring upper abdominal discomfort, back pain after meals, or unexplained digestive changes have become your normal, a proper gastro evaluation rules in or out the pancreas quickly.
At Gastro Plus, Dr. Vibhor Pareek offers:
- Pancreatitis diagnosis and management, acute and chronic, including severity staging
- ERCP (Endoscopic Retrograde Cholangiopancreatography), for bile duct and pancreatic duct evaluation and treatment
- Enzyme replacement therapy and chronic pain management for long-term cases
- Nutritional guidance specific to pancreatic conditions and post-flare recovery
- Advanced gastro diagnostics, imaging correlation, functional assessment, and targeted investigations
Book a Consultation at Gastro Plus
Frequently Asked Questions
Q1. Where exactly does it hurt when you have pancreatitis symptoms?
The pain typically sits in the upper middle or upper left abdomen, and its defining feature is that it radiates through to the back.
It’s not the diffuse cramping of gas or the lower abdominal discomfort of IBS, it’s a constant, deep ache in the upper region that worsens with meals and doesn’t shift or ease the way typical digestive pain does.
Q2. What feels like pancreatitis symptoms but is not?
Several conditions produce very similar symptoms, peptic ulcers, gallbladder attacks, GERD, and even left-sided kidney stones can mimic pancreatitis symptoms closely. Key distinctions:
- Gallbladder pain is typically sharper and more right-sided
- GERD rarely radiates to the back with this intensity
- Blood tests, specifically serum lipase and amylase, are what confirm pancreatitis; symptoms alone can’t
Q3. Is pancreatitis dangerous?
Mild acute pancreatitis resolves within days with proper management and is generally not life-threatening. Severe acute pancreatitis, however, can cause organ failure, infected pancreatic necrosis, or internal haemorrhage, requiring ICU-level care.
Chronic pancreatitis carries long-term risks including malnutrition, persistent pain, and diabetes development.
Q4. Can pancreatitis lead to diabetes?
Yes, especially in chronic cases where progressive pancreas inflammation damages the insulin-producing beta cells. This is called pancreatogenic or Type 3c diabetes and it behaves differently from Type 2:
- Oral medications are often less effective
- Insulin therapy tends to be needed earlier in the disease course
Q5. What should I eat if I have pancreatitis symptoms?
During an acute flare, the pancreas needs complete rest, start with clear liquids only and progress slowly under medical supervision. Long-term management:
- Low-fat diet (fat is the strongest trigger for digestive enzyme secretion)
- Small, frequent meals rather than large ones
- Complete alcohol avoidance, not moderation, avoidance
Q6. Can pancreatitis be prevented?
Completely preventing it isn’t always possible, particularly for hereditary or idiopathic cases. The most common triggers, however, are manageable:
- Treat gallstones before they cause a blockage, don’t wait for symptoms to worsen
- Avoid heavy or binge drinking, even occasionally
- Keep triglyceride levels in check through diet, exercise, and medication if needed