Living with IBS Means Living With Uncertainty — Especially Around Food:-
IBS is one of those conditions that colonizes your relationship with food. You stop eating things you love because you’re not sure what they’ll do to you. You plan meals around proximity to bathrooms. You eat something that was fine last Tuesday and this Tuesday it isn’t. The inconsistency is maddening. And the advice — ‘eat more fiber,’ ‘reduce stress,’ ‘try probiotics’ — feels frustratingly thin when you’re in the middle of a flare that’s derailed your day. Finding the right diet for IBS can make a major difference in managing symptoms like bloating, abdominal pain, diarrhea, and constipation.

A well-structured diet for IBS isn’t a cure. Let’s be honest about that upfront. There’s no single food plan that resolves IBS entirely for everyone. But dietary management is genuinely one of the most powerful tools available for reducing symptoms, and when it’s done properly — not just generically — it can significantly change how often and how severely symptoms show up.
A diet for IBS focuses on identifying foods that trigger digestive symptoms like bloating, abdominal pain, diarrhea, or constipation. The most effective approach is the low-FODMAP diet, which limits fermentable carbohydrates that irritate the gut. Personalizing food choices helps manage IBS symptoms more effectively.
Diet for IBS: Understanding How IBS Affects Your Gut
IBS (irritable bowel syndrome) is a functional gut disorder. The structure of the digestive tract is normal — no inflammation, no ulcers, nothing that shows up on imaging. What’s different is the function: gut motility is altered, the gut is hypersensitive to normal amounts of gas or distension, and the gut-brain communication is dysregulated in ways that make the system overreactive. Understanding the right diet for IBS begins with knowing how the digestive system behaves differently in people with irritable bowel syndrome.
This hypersensitivity is why certain diet for IBS cause disproportionate symptoms — bloating, cramping, diarrhea, constipation, or an alternating pattern of both. The digestive system is reacting to normal fermentation or distension as if it were a threat. Understanding this helps make sense of why some dietary changes work and others don’t.
The Low-FODMAP Diet — The Most Evidence-Backed Approach
The low-FODMAP IBS diet plan is currently the most rigorously studied dietary intervention for IBS. FODMAPs — fermentable oligosaccharides, disaccharides, monosaccharides, and polyols — are short-chain carbohydrates that are poorly absorbed in the small intestine. They travel to the colon where bacteria ferment them, producing gas and drawing water into the gut. The low-FODMAP approach is considered one of the most effective strategies when designing a diet for IBS.
For people with a hypersensitive gut, this process is amplified. The low-FODMAP approach works in three phases:
- Elimination phase (2 to 6 weeks): High-FODMAP foods are removed entirely to establish a baseline. If symptoms improve significantly, FODMAPs are confirmed as a driver
- Reintroduction phase (6 to 8 weeks): Individual FODMAP groups are reintroduced one at a time, in controlled amounts, to identify which specific categories cause symptoms and in what quantities
- Personalization phase (ongoing): The long-term diet is tailored to the individual’s specific tolerances — which are often more varied than a blanket ‘avoid all FODMAPs’ approach
This protocol should ideally be done with a registered dietitian who specializes in GI conditions. Self-directing it through a quick online FODMAP list tends to result in an unnecessarily restrictive long-term diet or incomplete reintroduction — neither of which serves you well.
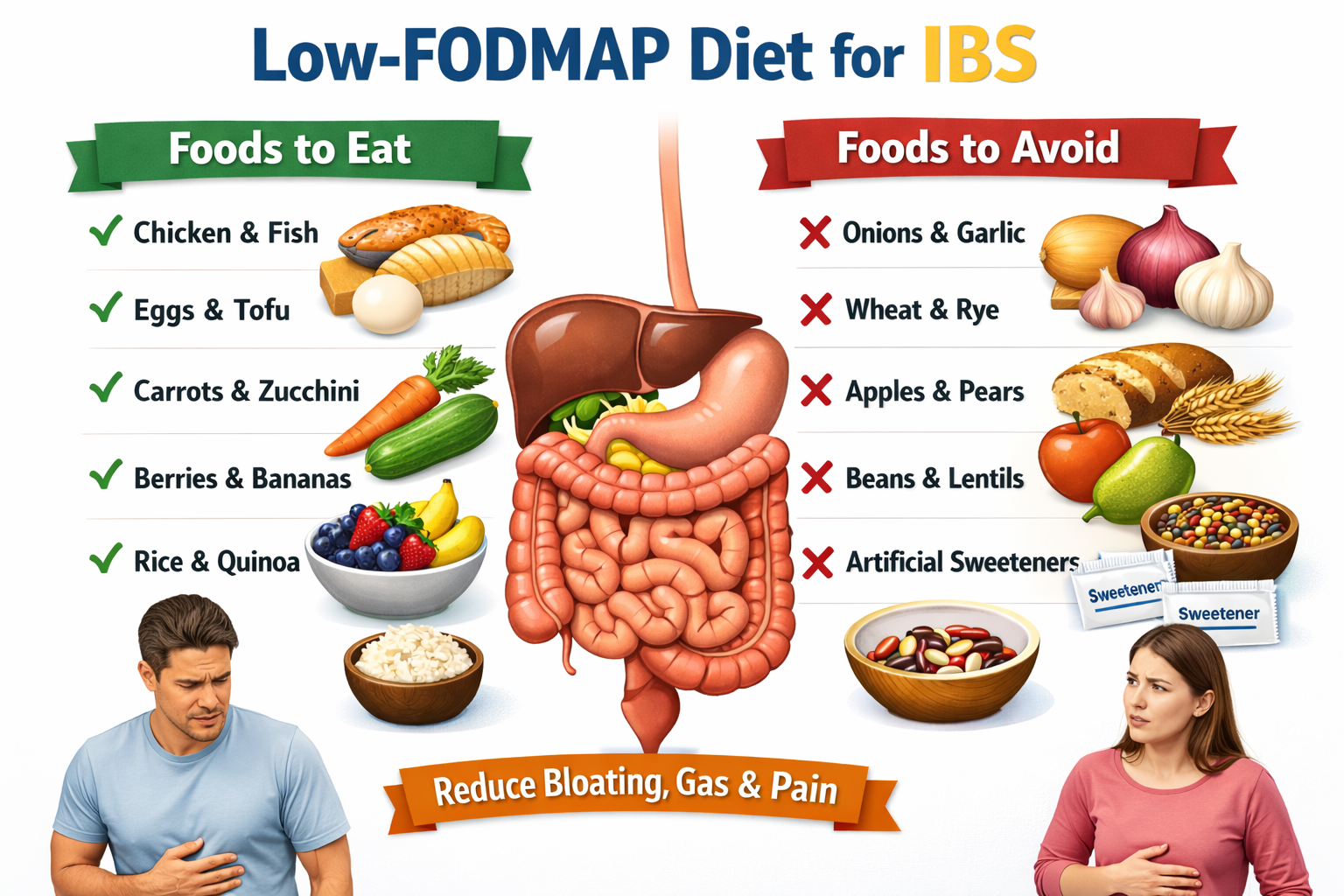
IBS Foods to Avoid — The High-FODMAP List
The common IBS food to avoid categories under the low-FODMAP approach. Identifying trigger foods is a key part of creating a personalized diet for IBS.
- Fructose-heavy foods — apples, pears, mangoes, honey, high-fructose corn syrup
- Lactose — regular milk, soft cheeses, ice cream, yogurt (hard aged cheeses are generally low-FODMAP)
- Fructans — wheat, rye, onions, garlic, leeks, asparagus. This is the category that surprises people most — onion and garlic are high-FODMAP even in small amounts
- Galactooligosaccharides (GOS) — legumes, lentils, chickpeas, cashews, pistachios
- Polyols — stone fruits (peaches, plums, cherries, avocado), mushrooms, cauliflower, and artificial sweeteners ending in ‘-ol’ like sorbitol, mannitol, xylitol
This doesn’t mean these foods are permanently off limits for everyone with IBS. The reintroduction phase often reveals that one or two FODMAP categories are the real culprits — not all of them. Many people discover they’re fine with lactose but react badly to fructans, or vice versa. The point is specificity, not blanket restriction forever.
What You Can Eat — Because the List Isn’t All Restrictions
The diet for IBS isn’t only about elimination. Low-FODMAP foods that are generally well-tolerated include: A balanced diet for IBS focuses on including well-tolerated foods while avoiding triggers.
- Most proteins — unprocessed chicken, turkey, fish, eggs, firm tofu
- Many vegetables — carrots, green beans, bell peppers, zucchini, spinach, cucumber, tomato in small amounts, eggplant, potatoes
- Many fruits — strawberries, blueberries, grapes, kiwi, oranges, bananas (just ripe, not overripe), pineapple
- Grains — rice, oats, quinoa, gluten-free pasta, sourdough bread (long-fermented sourdough reduces fructan content significantly)
- Lactose-free dairy, hard cheeses, almond milk, rice milk
- Nuts in moderate amounts — walnuts, pecans, macadamia nuts, almonds (small portions)
Fiber — Not All Types Are Equal for IBS
Fiber advice for IBS is often oversimplified to ‘eat more fiber.’ But the type of fiber matters enormously. Insoluble fiber — found in wheat bran, many whole grains — can aggravate IBS symptoms, particularly diarrhea-predominant IBS. It speeds up gut transit and increases mechanical stimulation of an already hypersensitive gut.
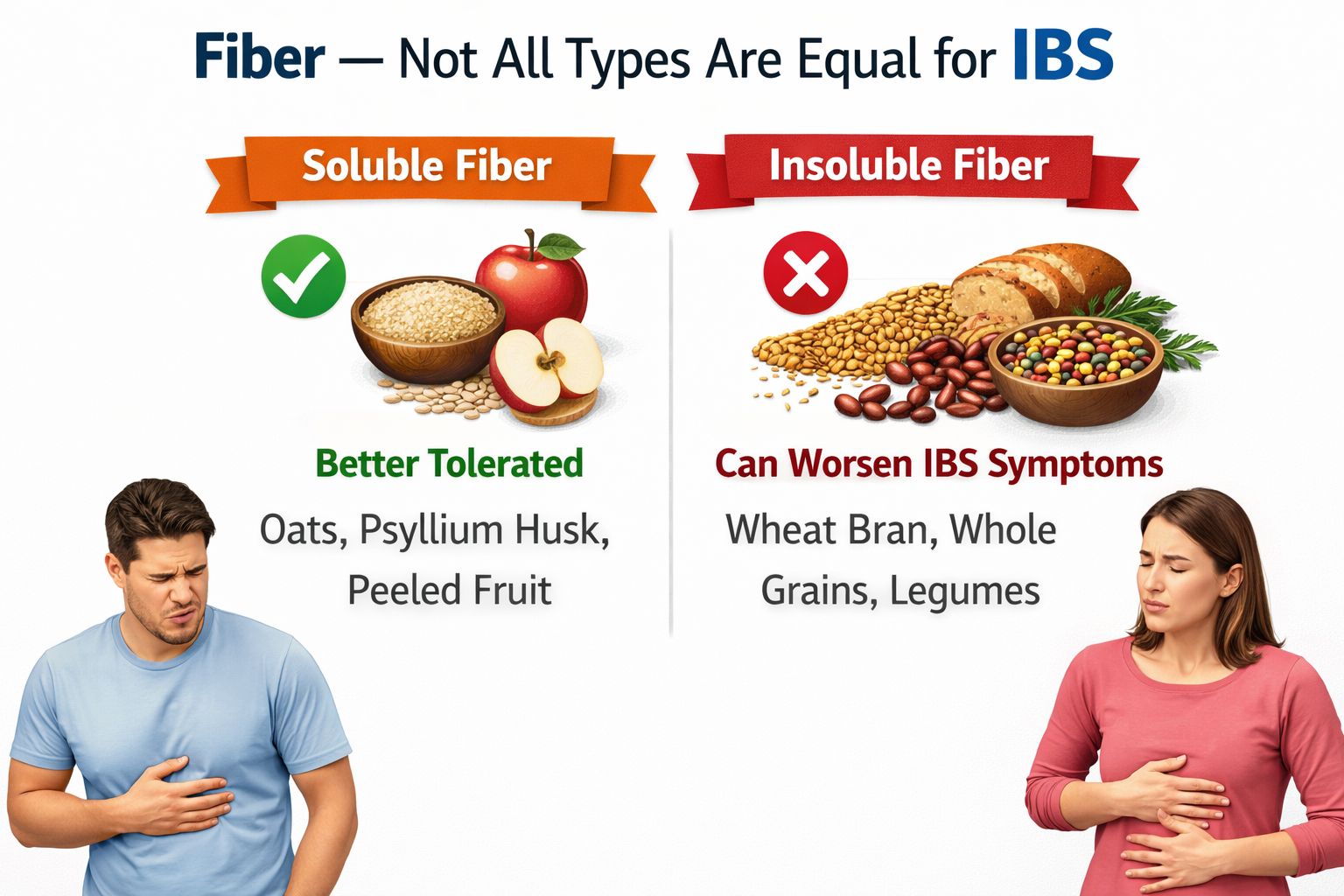
Soluble fiber is generally better tolerated and actually helps regulate stool consistency in both diarrhea-predominant and constipation-predominant IBS. Good sources: oats, psyllium husk (Metamucil), linseeds/flaxseeds, peeled fruits and root vegetables.
Psyllium husk in particular has solid clinical evidence for IBS symptom improvement and is one of the few supplements consistently recommended across subtypes.
Eating Habits Matter as Much as Food Choices
Following a structured diet for IBS also involves healthy eating habits and regular meal timing.
- Regular meal timing — irregular eating disrupts gut motility, which is already dysregulated in IBS. Three regular meals with planned snacks if needed works better than sporadic eating
- Smaller portions — large meals stimulate stronger gastrocolic reflex (the natural urge to empty the bowel after eating) and this reflex is amplified in IBS
- Eating slowly — less swallowed air, less distension, less unnecessary stimulation of the gut
- Adequate water intake — particularly important in constipation-predominant IBS; at least 1.5 to 2 litres per day
- Reducing alcohol and caffeine — both stimulate the gut; caffeine especially accelerates colonic transit which worsens urgency and loose stools in IBS-D
Poor dietary habits can also contribute to other digestive and metabolic conditions, including the early signs of fatty liver disease.
Probiotics and Supplements — The Real Picture
Probiotics get a lot of attention in IBS discussions. The evidence is genuinely mixed — some strains show benefit (Bifidobacterium infantis and certain Lactobacillus strains in particular), others show no effect, and strain specificity matters in a way that generic ‘probiotic’ supplement marketing doesn’t capture.
That said, they’re low-risk to try and some people see meaningful symptom improvement. A trial of two to four weeks with a quality multi-strain probiotic is reasonable.
Peppermint oil (enteric coated) has good clinical evidence for reducing IBS cramping and abdominal pain — better than many people expect from something so simple. Digestive enzymes can help if food intolerance (particularly lactase insufficiency) is contributing to symptoms.
Conclusion
The most effective diet for IBS is one that identifies personal food triggers while maintaining
balanced nutrition. The best diet for IBS for managing IBS symptoms is one that’s built around your specific triggers rather than a generic exclusion list. The low-FODMAP protocol, done properly, remains the most evidence-backed approach and often reveals that the problem isn’t ‘all high-FODMAP foods’ but a subset that’s specific to you. Soluble fiber, regular meal habits, reducing gut stimulants, and managing stress alongside diet — these are the pillars.
IBS doesn’t have to mean food fear. It can mean food intelligence — knowing your gut well enough to work with it rather than constantly being ambushed by it.
Frequently Asked Questions
- What is the best diet for IBS?
The low-FODMAP diet has the strongest evidence base for IBS symptom management. It involves eliminating fermentable carbohydrates that the gut poorly absorbs, then systematically reintroducing them to identify individual triggers. It’s best done with a GI-specialized dietitian to avoid unnecessary long-term restriction.
- What foods should I avoid with IBS?
High-FODMAP foods are the main targets: onions, garlic, wheat, apples, pears, legumes, dairy (for lactose-sensitive individuals), stone fruits, and artificial sweeteners. Alcohol, caffeine, very fatty foods, and spicy foods are also common irritants regardless of FODMAP content.
- Is gluten bad for IBS?
For most people with IBS, fructans (found in wheat, rye, and barley) rather than gluten itself appear to be the issue. This means many people improve on a low-FODMAP diet and tolerate gluten in low-fructan forms (like sourdough) without needing to be strictly gluten-free in the celiac sense.
- Can probiotics help with IBS?
Some probiotic strains show benefit in clinical trials — particularly Bifidobacterium infantis and certain multi-strain formulas. The evidence is inconsistent across strains and individuals. A 4-week trial of a quality probiotic is low-risk and worth trying, especially for IBS with bloating and altered bowel habits.
- How long does the low-FODMAP diet take to work?
Most people notice symptom improvement within two to four weeks of the elimination phase if FODMAPs are a significant driver. The full protocol including reintroduction typically takes three to four months. The goal is not to stay on a restricted diet permanently but to identify your specific tolerances.